Foot and Ankle Ice & Heat Wrap
Foot and Ankle Ice & Heat Wrap

FREE EXPRESS
SHIPPING

EASY
RETURNS

1-YEAR
GUARANTEE

HEAT & COLD
THERAPY
COMPRESSION

FLEXIBLE
WHEN FROZEN
PT DESIGNED

REUSABLE
PACKS
U.S. OWNED &
OPERATED
Regular price
$32.95 USD
Sale price
$32.95 USD
Unit price
per
Shipping calculated at checkout.
Couldn't load pickup availability
Details
Details
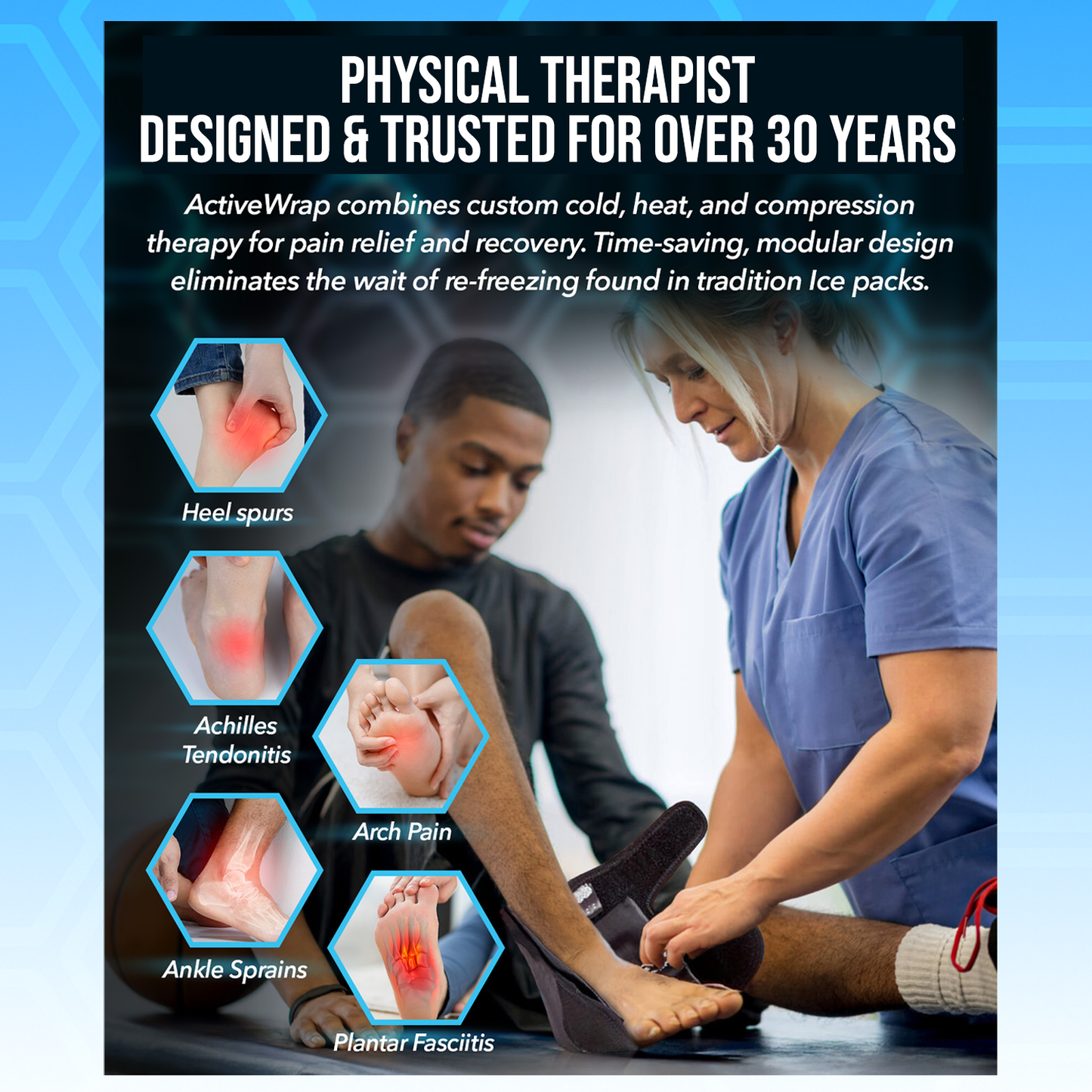
The ActiveWrap® Foot and Ankle & Ice & Heat Wrap is a physical therapist–designed solution for fast, targeted relief from ankle sprains, achilles tendonitis, plantar fasciitis, heel spurs, post-surgical pain, and more. Featuring two reusable ultra flex heat and ice packs and an adjustable compression wrap, it delivers customizable hot or cold therapy that stays soft, pliable, and in place for consistent comfort. Engineered for easy self-application, mobility, and a universal fit for either foot, the wrap molds to your foot and ankle for soothing, mess-free relief—making it an essential recovery tool for athletes, active lifestyles, and anyone managing foot or ankle pain.
SIZING
SIZING
How to use
How to use
Shipping information
Shipping information
MEDICAL DISCLAIMER
MEDICAL DISCLAIMER